Airway management
If there is potential that the patient’s airway may deteriorate due to injuries or respiratory insufficiency, intubation prior to retrieval should be discussed with the ARV consultants.
Assess adequacy of oxygenation and ventilation. Frequent reassessment of the patient must take place as injury sequelae may cause further airway compromise. In an intubated patient, end-tidal carbon dioxide (ETCO2) monitoring (if available) should be used to assess respiratory status and the adequacy of ventilation. Always have emergency airway equipment by the bedside.
Fluid resuscitation
IV fluids, usually normal saline. Order intravenous (IV) fluids, usually normal saline initially (until other trauma is excluded) then transfer to maintenance fluids.
Avoid fluid overload in the presence of neurogenic shock – use urinary output as the indicator and monitor fluid balance.
It is important to maintain an accurate fluid balance chart from the early stages of treatment to assess the effectiveness of fluid resuscitation. This will also assist retrieval staff with further management during transfer.
A general guide is to maintain a systolic blood pressure of above 90mmHg and targeting a MAP of 85-90mmHg.(15, 16) However, in setting of multi trauma / TBI these targets need to be altered to account for other pathologies.
Monitoring
Monitoring of the heart rate, respiration rate, blood pressure, temperature and oxygen saturation should take place at 15-minute intervals or more frequently if indicated. Monitor continuously via electronic monitoring if the facilities are available. All monitoring should be maintained until the retrieval team arrives.
A baseline ECG should be taken prior to transfer if time permits and facilities exist.
Expect hypotension and bradycardia associated with spinal shock in those with lesions at or above T6 neurological level of injury. The pulse commonly falls to 55 bpm or less. Blood pressure often falls to 90 mmHg systolic. A heart rate less than 45 bpm and blood pressure less than 90 mmHg require treatment in consultation with ARV and the receiving spinal unit or trauma service.
Ongoing assessment of the patient’s neurological function is indicated to assess for symptom extension due to ascending spinal cord oedema.
Medical imaging
Radiological examination is crucial in the diagnosis of SCI.
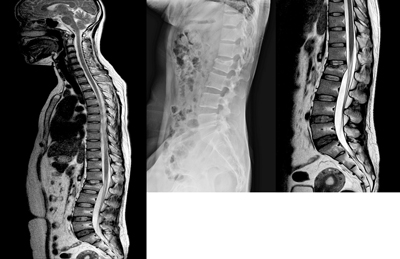
Plain x-rays may provide initial information on spinal injury, however, are not used to clear the trauma patient of injury. The patient should be cared for as a possible cervical vertebral injury.
A CT scan/MRI should be undertaken if the NEXUS criteria for cervical spine clearance have not been met, or the patient is unconscious. Should the patient exhibit any of the criteria as mentioned previously, then clinical examination is unreliable and radiographic assessment is advised. Where facilities do not have CT imaging available, then consultation with ARV and the MTS regarding retrieval and transfer should take place. X-ray imaging of the cervical spine is not suitable to clear the neck of the trauma patient. It may be appropriate to delay exhaustive imaging investigations if they are not going to alter management. Definitive imaging may be performed at the receiving specialist unit.
All SCI patients must have a chest x-ray. If head trauma or loss of consciousness has occurred, a CT brain is indicated. Consider further diagnostic imaging if available and indicated.
Wound care
All wounds should be covered with a suitable and secure occlusive or dry dressing.
All other injuries / wounds should be appropriately managed.
Pressure area care
Special attention should be paid to pressure area care and surveillance in consideration of the extended time that spinal patients may remain supine.
Importantly if equipment is available, an appropriately sized, rigid foam, soft collar should ideally be fitted as soon as possible or within 6 hours of injury.
Analgesia
Opioids are the drug of choice in the acute SCI management phase. IV administration is the most effective route due to its rapid absorption, for both adults and children. Administer as per local protocols and titrate to effect.
Strongly consider anti-emetics at this stage, especially if transfer and retrieval is anticipated.
Minimise Heat Loss
It is important to maintain normothermia. Patients with high SCI present with poikilothermia, where normal thermoregulation is compromised, and hypothermia becomes a concern.
If available, the use of a forced air-warming machine is encouraged. Ensure wound care is attended to before commencing. Re-assess the room temperature at regular intervals while awaiting the retrieval team.
Glasgow Coma Scale
A focused neurological assessment using the GCS should be performed (see table below). This should include a description of the patient’s level of consciousness as well as assessments of pupillary size and reactivity, gross motor function, and sensation. Document the findings and reassess at frequent intervals.
| Best response | Eye opening | Verbal response | Motor response |
| 1 | Does not open eyes | Makes no sounds | Makes no movements |
| 2 | Opens eyes in response to painful stimuli | Incomprehensible sounds | Extension to painful stimuli (decerebrate response) |
| 3 | Opens eyes in response to voice | Utters inappropriate words | Abnormal flexion to painful stimuli (decorticate response) |
| 4 | Opens eyes spontaneously | Confused, disoriented | Flexion or withdrawal to painful stimuli |
| 5 | N/A | Oriented, converses normally | Localises painful stimuli |
| 6 | N/A | N/A | Obeys commands |
Pathology
Pathology tests should be taken for FBC (full blood count), UEC (urea, electrolytes and creatinine) and glucose as well as a blood gases if available. Consider taking a group and cross-match if the patient is involved in a trauma presentation with a high index of suspicion for further injuries.
In-dwelling catheter
A urinary catheter should be inserted, and urine output measured hourly. The desired urine output for adults is 0.5-1.0 mL/kg/hr.(21)
A urinalysis should also be performed to check for blood.
Naso/orogastric tube (N/OGT)
All patients should be kept nil orally in the initial post-resuscitation phase of injury.
NGT insertion should be considered for managing paralytic ileus in spinal-injured patients, and must be placed for all SCI retrieval/transfers.
The potential for a base of skull fracture in polytrauma should be considered as a relative contraindication in the decision to insert an NGT. An OGT may be inserted following consultation and under direct visualisation.
Antibiotics
Routine antibiotic administration is not recommended in the initial phase of trauma injury management.
Reassess
The importance of frequent reassessment cannot be overemphasised. Patients should be re-evaluated at regular intervals as deterioration in a patient’s clinical condition can be swift. This will be evident in their vital signs and level of consciousness. If in doubt, repeat the primary survey.
Other
Steroids are not routinely recommended in SCI.