The primary survey is the initial assessment and management of a trauma patient.
Use a systematic approach based on <C> ABCDE (7, 8) to assess and treat an acutely injured patient. The goal is to manage any life-threatening conditions and identify any emergent concerns.
- Catastrophic haemorrhage
- Airway with in-line spinal immobilisation
- Breathing
- Circulation
- Disability (neurological)
- Exposure and environment
On arrival to the emergency department, the patient should have full non-invasive monitoring applied, and initial management including:
- ECG monitoring.
- Non-invasive blood pressure cuff.
- Oxygen saturation probe.
- The patient’s temperature should be recorded.
- Removal of the patient’s clothes is encouraged so that they can be fully assessed.
- Oxygen should be applied to achieve saturation of 94-98%
In single responder settings these may need to be addressed in a linear or sequential fashion; however, when a team is assembled, these elements may be addressed simultaneously. The term ‘survey’ is somewhat misleading in that it implies that only assessment is occurring; however, each phase requires simultaneous assessment for, and management of, any life threats detected.
Catastrophic Haemorrhage
Assess for catastrophic haemorrhage
- Identify any large volume external blood loss.
- Provide immediate management as required, consider; direct pressure, haemostatic dressings and torniquets.
Failure to recognise and control large-volume external haemorrhage significantly increases mortality. Obvious large volume external blood loss must be managed as an immediate priority in the field and on arrival of the patient into the emergency department, with the aim being to control life-threatening external haemorrhage (10, 11).
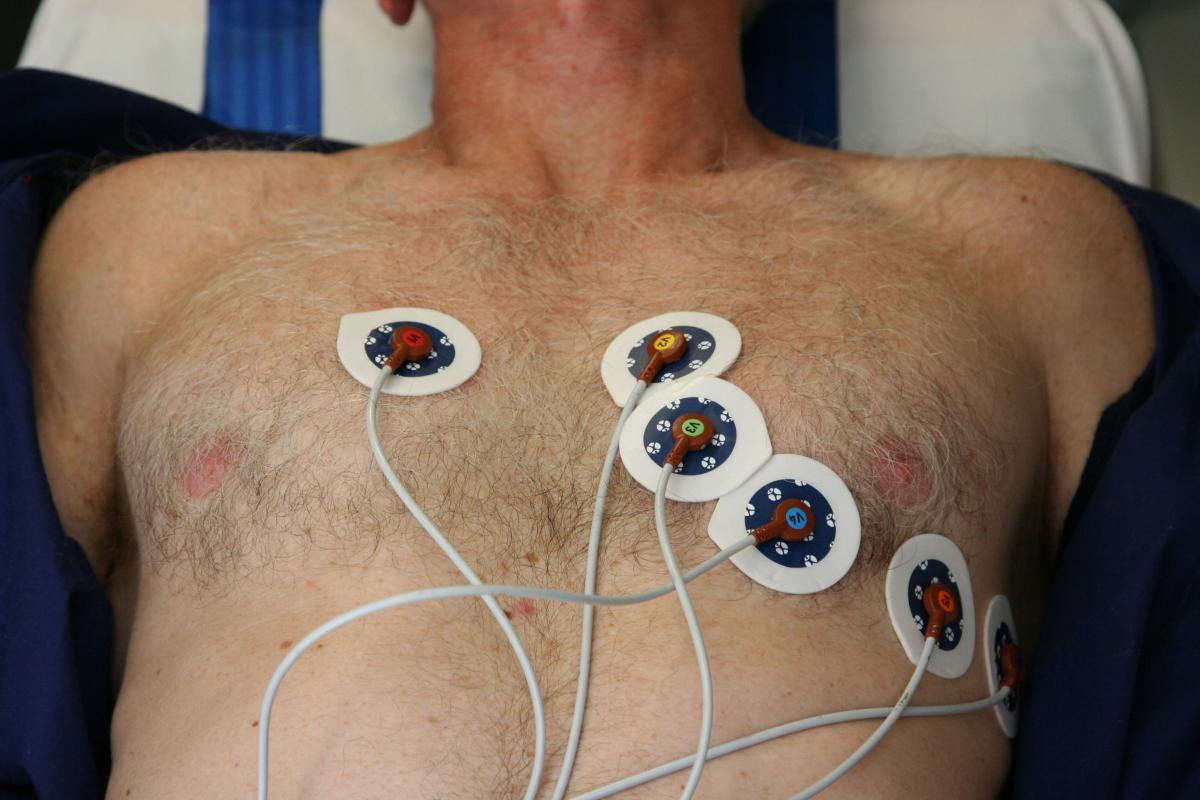
Image used with permission from Department of Health, Victoria
Airway with cervical spine protection
An assessment of airway patency and stability should be performed during the primary survey and a plan for airway management instituted if required. Unless the patient is in cardiac arrest, immediate securing of the airway with endotracheal intubation is rarely required upon arrival of a major trauma patient.
Life threats
The following airway life threats must be assessed and managed:
- Airway obstruction.
- Blunt or penetrating neck injury.
- Reduced conscious state.
Assess for airway stability:
- Attempt to elicit a response from the patient.
- Look for signs of airway obstruction (use of accessory muscles, paradoxical chest movements and see-saw respirations).
- Listen for signs of upper-airway noises and breath sounds. Are they absent, diminished, or noisy?
- Assess for displaced dentures, especially in the older persons cohort.
Assess for soiled airway
- Haemorrhage, vomiting or excessive secretions should be removed with suction.
- If there is excessive bleeding into the airway that cannot be removed with suction, it may be necessary to manage the patient on their side to allow drainage of blood from the mouth or nose, while maintaining C spine immobilisation. Patients can be placed on their side by performing a log-roll manoeuvre.
- If this is insufficient consideration should be given to sitting the patient upright. The risk of potential spinal injury must be weighed against the potential for complete airway obstruction or choking from aspirated blood.
- If there is uncertainty about the safety of this, a senior doctor with airway experience should be involved or the ARV clinician can be contacted for advice or for telehealth review of the situation.
Attempt simple airway manoeuvres if required:
- Open the the airway using a chin lift and jaw thrust whilst avoiding neck extension in order to protect the C-spine.
- Suction the airway if excessive secretions are noted or if the patient is unable to clear their airway independently. Prolonged suctioning can lead to an increase in intracranial pressure (ICP) so be mindful to limit duration (12, 13).
- Insert an oropharyngeal airway (OPA)/nasopharyngeal airway (NPA) if required.
- Care should be taken to not extend the cervical spine.
Caution: NPA should not routinely be inserted in patients with a head injury in whom a base of skull fracture has not been excluded (14, 15). In the setting of airway obstruction, or failure to oxygenate, then an NPA can be inserted if delay to definitive airway management.
Caution: Rapid-sequence intubation in patients with blunt or penetrating neck injuries carries the risk of total loss of airway patency upon administration of sedative and/or muscle relaxant medication.
If the patient is already intubated, document the size and position of the endotracheal tube, including lip level, end-tidal carbon dioxide trace, cuff pressure and any intubation difficulty (or Mallampati score). Where possible, delegate ongoing airway management to an airway doctor/nurse and continue the initial assessment.
Secure the airway if necessary (treat airway obstruction as a medical emergency)
- Consider intubation early if there are any signs of:
- A decreased level of consciousness, unprotected airway, uncooperative /combative patient leading to distress or further risk of injury.
- Hypoventilation, hypoxia or a pending airway obstruction, indicated by signs such as a stridor or hoarse voice.
Maintain full spinal precautions if indicated
- Suspect spinal injuries in all polytrauma patients. Ensure a cervical collar, head blocks or in-line immobilisation is maintained throughout patient care.

Breathing and ventilation
Life threats:
- Tension pneumothorax.
- Massive haemothorax.
- Open pneumothorax.
- Flail chest and Pulmonary contusions.
- Tracheobronchial injury.
Oxygen administration
All patients with chest injuries have a high oxygen demand and therefore supplemental oxygen should be supplied until injury is excluded or effectively managed. Make sure to check the back also as life threatening injuries may be otherwise undetected. Immediately after detection of any life-threatening injuries, interventions need to occur to prevent further deterioration.
- Administer oxygen to achieve oxygen saturations between 94-98%.
Assess the chest
The chest should be fully exposed and inspected:
- Note respiratory rate / effort / SpO2.
- Look for open wounds / penetrating wounds / tracheal deviation
- Observe any bruising / deformity / abnormal chest movements, e.g., intercostal and / or supraclavicular in-drawing.
- Palpate: Tenderness, crepitus, surgical emphysema.
- Auscultate chest for bilateral air entry, additional noises.
A mobile chest x-ray should be performed in the resuscitation bay at the earliest opportunity and performed with a pelvic x-ray during the primary survey.
If a tension pneumothorax is suspected, management should include:
- Emergent decompression using a 14G needle in the second intercostal space in the mid-clavicular line. This is completed if equipment and skilled personnel for finger thoracostomy is not immediately at hand (16).
- Finger thoracostomy with blunt dissection and digital decompression through the pleura is the preferred treatment option. Decompression of the pleural space is a primary goal during the reception and resuscitation of the haemodynamically unstable patient with a haemothorax and/or pneumothorax (17).
- Intercostal catheter insertion. Finger thoracostomy should be followed by the insertion of an intercostal catheter connected to an underwater seal drain as a secondary priority that can be completed at a later stage.
Note: Finger thoracostomies require definitive ongoing management with an ICC unless the patient is positive pressure ventilated.
Record the oxygen saturation (SpO2) and ETCO2 if available.
This will provide trends for the patient as well as being a precursor to any change in condition or deterioration.

Circulation with haemorrhage control
Assess circulation and perfusion
Circulation assessment in major trauma focuses on detecting and managing shock, or reduced tissue perfusion. The most common cause of shock in a major trauma patient is hypovolaemic shock from blood loss. Blood loss may be external/visible, and therefore compressible, or internal/concealed and non-compressible.
- Pulse – Quality/ rate/ regularity
- Skin – colour / cap refill time / temperature
- BP
- JVP – raised/ flattened.
- Perform eFAST scan looking specifically for evidence of pericardial tamponade, pneumothorax, haemothorax and intraperitoneal free fluid.
Intravenous access
Insert two large-bore peripheral intravenous (IV) cannulas. If access is difficult, consider obtaining central access or proceed to intraosseous insertion if the equipment/skills are available.
eFast scan
In experienced hands eFAST (Extended Focused Assessment with Sonography in Trauma) has a high sensitivity and specificity (18). It supplements physical examination for detecting intra- thoracic and intra-abdominal injury (19). In the hypotensive patient, eFAST should be performed as part of the primary survey. In penetrating trauma to the torso an eFAST should be performed in all cases. In patients who are haemodynamically stable the eFAST may be delayed until the secondary survey if resources do not permit.
Further haemorrhage control
Control of catastrophic haemorrhage should have been completed as the first step of the primary survey. If there is any other external haemorrhage that is now found, it will require further management.
- Where external haemorrhage is identified an attempt must be made to control it using direct pressure, dressings, elevation and if uncontrolled then a proximal tourniquet should be utilised, if available.
- Smaller injuries (for example, puncture wounds) that are bleeding excessively should be managed by direct, local pressure over the wound with 10 cm × 10 cm gauze squares folded in half and folded again to make a 5 cm × 5 cm gauze pad, and placed over the wound with firm, single digit pressure. This will control haemorrhaging better than loosely applied, large absorbent pads. It is helpful to take photos of the wounds and injuries to assist with ongoing management plans at the receiving facility.
- It is best to avoid suturing or stapling wounds closed prior to transfer, unless the haemorrhaging cannot be controlled with direct pressure. If wounds are closed purely for haemostasis, this must be documented in the clinical record and communicated to the receiving team as they may need to be re-opened and/or explored on arrival at a receiving hospital.
- If there is suspicion of pelvic injury, an appropriate pelvic binder should be applied if not already in-situ. A pelvic binder is important in controlling and minimising further haemorrhage.

Image used with permission from Department of Health, Victoria

Disability
Assess level of consciousness
- Complete an AVPU assessment (Alert, responds to Voice, responds to Pain, Unresponsive). A more detailed neurological assessment using the GCS will be performed in the secondary survey.
Check pupillary size and responses
- Unequal or unresponsive pupils may be an indication of severe TBI and raised intracranial pressure. It will be important to note if the pupils change during the patient’s re-assessments.
Test blood sugar levels
- Ensure that any alterations in the patient’s level of consciousness are not related to a metabolic cause. Identify and correct hypoglycaemia.

Exposure and environment

By the end of the primary survey the patient should have been fully exposed to ensure no injuries posing an immediate life threat are overlooked. Consideration must be given with respect to their age, gender, and culture. All patients should be exposed appropriately and sequentially, exposing one body region at a time whilst attempting to preserve patient dignity. Prior to exposing a patient, the patient should be informed, and consent should be gained where possible.
- Remove all clothing from the patient and assess to ensure there are no other obvious, life-threatening injuries present.
- Keep the patient normothermic through passive re-warming with blankets and a warm environment.